Superior Mesenteric Artery (SMA) and Celiac Artery aneurysms are rare but potentially life-threatening vascular conditions characterized by abnormal dilations of the SMA or celiac artery walls. These aneurysms can lead to catastrophic complications such as rupture, hemorrhage, or ischemia of vital abdominal organs. Early recognition and appropriate management are crucial to prevent morbidity and mortality. This article provides a detailed exploration of SMA and celiac artery aneurysms, covering anatomy, causes, clinical presentation, diagnosis, treatment options, and prognosis.
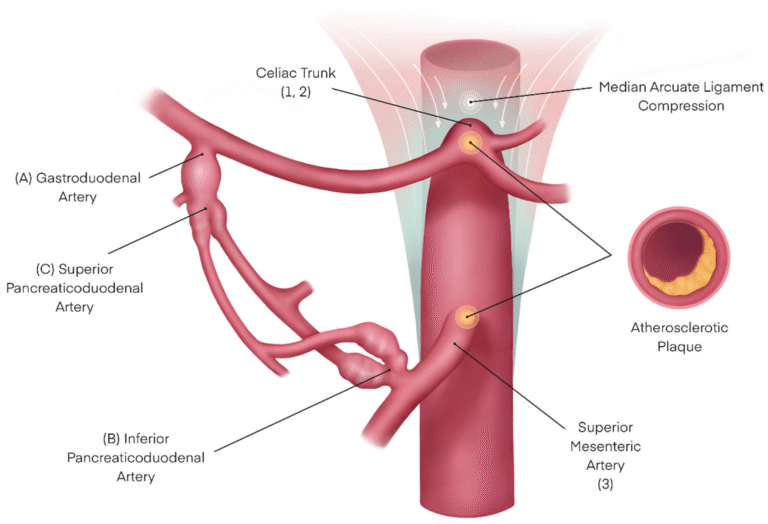
The celiac artery and superior mesenteric artery (SMA) are major branches of the abdominal aorta supplying blood to the upper abdominal organs.
An aneurysm is a localized dilation of an artery exceeding 1.5 times its normal diameter. SMA and celiac artery aneurysms are uncommon compared to aortic aneurysms but carry significant risk due to their proximity to vital organs and potential for rupture.
Several factors contribute to the development of SMA and celiac artery aneurysms:
Many SMA and celiac artery aneurysms are asymptomatic and discovered incidentally during imaging for other reasons. When symptoms occur, they may include:
Because symptoms are nonspecific, high clinical suspicion is necessary, especially in patients with risk factors.
Diagnosis involves a combination of clinical evaluation and imaging studies:
Management depends on aneurysm size, symptoms, risk of rupture, and patient comorbidities.
Indicated for:
Options include:
Seek immediate medical attention if you experience:
Regular check-ups are advised for individuals with known risk factors or previous aneurysms.
SMA and celiac artery aneurysms, though rare, pose significant health risks due to their potential for rupture and organ ischemia. Understanding the anatomy, causes, symptoms, and diagnostic methods is vital for timely intervention. Treatment ranges from careful monitoring to complex surgical or endovascular repair, tailored to individual patient needs. Early consultation with vascular specialists and adherence to follow-up protocols can greatly improve prognosis. If you suspect any symptoms or have risk factors, consult a healthcare professional promptly to ensure optimal care and outcomes.

Aenean porta orci nam commodo felis hac ridiculus fusce fames maximus erat sed dictumst blandit arcu suspendisse sollicitudin luctus in nec
